Between the ongoing COVID-19 pandemic, a new baby, a move and starting two new jobs, I haven’t had the time to keep this website going (as I am sure many have noted). The COVID-19 page has not been updated but at this time, there are plenty of other resources available that summarize the relevant and updated literature.
As of now, I am not sure when I will have the time to dedicate to this site. However, I do plan to get back to it one of these days. In the meantime, its my 2022 New Years resolution to remain more active on Twitter (@foamid) and continue to bring small clinical ID pearls. See you there!
There’s so much information about the novel coronavirus COVID-19 on the internet that it is hard to keep up with the onslaught of information. We wanted to compile the ultimate list of reputable resources for clinical providers to access when they need to, at a moment’s time.
Since information on COVID-19 is rapidly changing, these resources are not specific papers or blog posts, but rather websites that are maintaining up to date information on epidemiology, pathophysiology, and management. Resources span all types, including website behemoths like the WHO and CDC, as well as twitter accounts for people who get their news from social media.
Since this is an ultimate list but we don’t pretend to have ultimate knowledge of all resources, please send us resources that we may have missed and we will add them on here! We also acknowledge that this list is U.S. centric because we are from the States, but we would love input on resources for other countries so we can make this a more international list.
Sanford Guide – quick but detailed practical clinical overview of everything you need to know about COVID-19 when you’re taking care of patients with COVID-19
Infectious Diseases Society of America – resource center includes clinical guidelines, recommendations, and up to date payment coverage (!) for COVID-19 treatment
University of Washington – the holy grail of practical documents developed by people who are currently battling a COVID-19 outbreak. All documents can be utilized by others and adapted for their own institutional protocols.
IDStewardship – a very thorough, but easily read overview of potential treatment options for COVID-19 and how/when to use them
University of Liverpool – charts on drug drug interactions with experimental therapies for COVID-19
CIDRAP – focuses on the health policy aspect of COVID-19 news
Society of Critical Care Medicine – online training modules for disaster medicine, resource availability in U.S., and other fantastic resources for front-line clinical providers
ClinicalTrials.gov – a currently-recruiting randomized controlled trial of remdesivir for COVID-19 treatment
CURE ID – an FDA and NIH supported website where you can report and see new uses of existing drugs for difficult-to-treat infectious diseases. Download their mobile app too!
Blogs:
Virology Blog– blog run by virologists with recent discussions on COVID-19
ScienceSpeaks– global ID news blog written by physicians
ChasingMicrobes.com – a weekly update on COVID-19 literature compiled by the Boston Children’s Hospital pediatric Infectious Diseases fellows
This Podcast Will Kill You – Two epidemiologists (both named Erin) provide you with an entertaining summary of new COVID-19 knowledge, alongside a recipe for a Quarantini and a Placeborita.
[This post was written by Ahmed Abdul Azim, a senior infectious disease fellow at Beth Israel Deaconess Medical Center]
During the fall and winter season, you are likely to see a few cases of viral meningitis. Even though viral encephalitis is less common, it is important to try to differentiate these clinical entities as a clinician, since they carry different prognoses. (The bulk of this review is adapted from Mandell, Douglas and Bennett’s principles and practice of infectious diseases)1
Cerebral spinal fluid analysis
Before we go any further, let’s briefly review cerebral spinal fluid findings on lumbar puncture for different syndromes:
WBC(cells/mm3)
Primary cells
Glucose(mg/dL)
Protein(mg/dL)
Viral
50-1000
Lymphocytic
>45
<200
Bacterial
1000-5000
Neutrophilic
<40
100-500
Mycobacterial
50-500
Lymphocytic
<45
50-300
Cryptococcal/fungal
20-500
Lymphocytic
<40
>45
Important points to consider: · Bacterial meningitis: 10% of cases have a lymphocyte predominant CSF cell analysis · WNV encephalitis: over a 1/3 of patients with WNV encephalitis had neutrophil predominant CSF pleocytosis · Enteroviruses: CSF analysis done early in illness course may yield neutrophil predominant pleocytosis in 2/3 of cases – generally will convert to lymphocytic predominant if repeated in 12-24 hours.
Take home point: always interpret CSF within the clinical context in front of you!
CSF to serum glucose ratio of < 0.4 is suggestive of bacterial meningitis
Traumatic LP may cause elevated CSF protein: for every 1000 RBC/mm3, subtract 1 mg/dL protein
Traumatic LP may cause elevated CSF WBC: for every 500-1000 RBC/mm3, subtract 1 WBC/mm3
RBC Adjustment for WBC in CSF = Actual WBC in CSF – (WBC in blood x RBC in CSF/RBC in blood)
Viral meningitis versus encephalitis
Both syndromes often present with a triad of2: (1) FEVER (2) HEADACHE and (3) ALTERED MENTAL STATUS However, the trick is to explore the history and signs further. Epidemiological clues include:
travel history
prevalence of disease in the local area
occupational exposure
animal and insect exposure
immunization history
underlying immune status
Patients with viral encephalitis: tend to have diffuse cerebral cortex involvement with abnormal cerebral function – Symptoms: altered mental status, motor/sensory deficits, altered behavior and/or personality changes, speech and/or movement disorders
Patients with viral meningitis: DO NOT have diffuse cerebral cortex involvement → cerebral function IS INTACT – Symptoms: headache, lethargy, neck stiffness/pain
Patients with meningoencephalitis: tend to have a combination of meningitis and encephalitis symptoms
Regardless, if a patient has symptoms and/or signs of meningitis or encephalitis, a lumbar puncture can be helpful.
Viral Meningitis – Common Pathogens
Overall, most cases of aspectic meningitis syndromes are caused by viruses
1. Enteroviruses (e.g. Coxsackie, echovirus, other non-polio enteroviruses) – by far the most common cause of viral meningitis/aseptic meningitis3
Summer/fall seasons (less commonly in the winter)
Clinical manifestations:
abrupt onset fever
headache
vomiting/diarrhea
photophobia
malaise
+/- meningismus
Think of enterovirus viral meningitis in patients when rash and/or diarrhea is present
CSF analysis done early in illness course may yield neutrophil predominant pleocytosis in 2/3 of cases – generally will convert to lymphocytic predominant if repeated in 12-24 hours4.
Take home point: always interpret CSF within the clinical context in front of you!
2. Herpes virus simplex viral meningitis – usually caused by HSV-2 >> HSV-18
Only accounts for 0.5-3% of viral meningitis/aseptic meningitis cases9
Typically mild symptoms
80% with HSV-2 genital lesions/ulcers up to 1 week prior to presenting with viral meningitis
Patients with a clinical picture consistent with aseptic meningitis and have HSV isolated in CSF will end up having HSV-2 in 95% of cases. This is a self-limited illness3
3. West Nile Virus – more likely to cause an encephalitis syndrome. Yet, may present with aseptic meningitis or asymmetrical flaccid paralysis10
Viral Encephalitis – Common Pathogens
A cause is identified in approximately 36-63% of cases10,11
Causes of encephalitis (Most common to least common in US study of patients that met criteria for encephalitis)12:
Viruses (70%)
Enteroviruses: 25%
HSV-1: 24%
Varicella zoster virus (VZV): 14%
West Nile virus (WNV): 11%
EBV: 10%
Others: 16%
Bacteria (20%)
*In a study of HIV uninfected patients, viruses caused up to 38% of cases, followed by bacterial pathogens at 33%, Lyme disease at 7%, and fungi at 7%. Syphilis was identified as the culprit in 5% of cases, and mycobacterial infections at 5%, while prion disease was responsible for 3% of cases of encephalitis11
1. HSV encephalitis: most common cause of encephalitis in the US (1/250,000 population annually). HSV-1 accounts for greater than 90% of HSV encephalitis in adults13. Fewer than 6% of CSF PCR cases had a “normal” neurological exam14.
> 96% have CSF pleocytosis14,15,16
Protein is elevated; glucose is normal 95% of the time14,15,16
MRI > CT, revealing changes of temporal lobes in ~89% of cases confirmed by CSF PCR15
CSF PCR is highly sensitive and specific, with an excellent positive and negative predictive value17
If HSV encephalitis is suspected and PCR is negative, repeat HSV PCR testing in 3-5 days
HSV PCR remains positive up to 7 days in 98% of cases after onset of symptoms
Treatment: IV acyclovir is the treatment of choice; call your nearest ID colleague for help
Mortality in acyclovir-treated patients stratified by age group18:
11% in < 2 year olds
22% in 22-59 year olds
62% in > 60 year olds (initial level of consciousness strongly predicted mortality16)
2. West Nile Virus encephalitis: transmitted via a mosquito (vector) bite, currently the most common cause of epidemic viral encephalitis nationally19
Most are asymptomatic (80%); macular rash in up to 50% of cases20
<1% develop neuroinvasive disease, of which 60% develop encephalitis21
High risk patients for neuroinvasive disease: solid organ transplant patients22
Clinical presentation21
Fever: 70-100%
Headache: 50-100%
Encephalopathy: 45-100%
Cranial neuropathies, mostly facial palsy: 20%
Lower motor neuron type lesion: areflexia, hypotonia, preserved sensation
Tremors are not uncommon either
CSF analysis: pleocytosis (>60% of cases lymphocytic predominant), elevated protein and normal glucose13
WNV encephalitis will likely have neuroimaging findings; that is not the case with WNV meningitis
MRI much more sensitive than CT. Most common abnormalities seen involving basal ganglia, brain stem and thalamus1
CSF diagnosis: WNV-specific IgM in CSF23
No established therapy for neuroinvasive disease. Case reports of improvement with IVIG for neuroinvasive disease1
Mortality: 12% in severe neuroinvasive disease. Residual neurological changes such as parkinsonism not uncommon
Approximately 30% of patients reported fatigue symptoms 6 months to 5 years after infection onset24
Viral Meningoencephalitis – Clinical Approach
So you are the house officer encountering a patient with 1-2 weeks of progressively worsening fevers, headaches and severe behavioral changes or depressed mental status: what do you do next?
As a standard work up for likely encephalitis in the United States, CSF studies should include1:
CSF opening pressure
Cell count and differential
Protein and glucose (paired with serum glucose)
Gram stain and bacterial cultures
Initial viral studies to include:
HSV-1/2 PCR;
VZV PCR;
Enterovirus PCR;
WNV IgM serology (if seasonally appropriate);
CSF viral cultures
Imaging in encephalitis: Magnetic resonance imaging (MRI) of the brain is more sensitive than computed tomography (CT)15. Unless contraindicated, all patients with encephalitis should undergo MR imaging.
Temporal lobe and limbic changes → HSV, HHV-619
Hemorrhagic strokes and demyelinating lesions → VZV vasculopathy25
Subependymal enhancement → CMV ventriculitis25
Predominant demyelination → PML (JC virus)
References:
1. Mandell, Douglas and Bennett’s principles and practice of infectious diseases (8th ed. 2015 / Philadelphia, PA : Elsevier) 2. Whitley RJ, and Gnann JW: Viral encephalitis: familiar infections and emerging pathogens. Lancet 2002; 359: pp. 507-513 3. Connolly KJ, and Hammer SM: The acute aseptic meningitis syndrome. Infect Dis Clin North Am 1990; 4: pp. 599-622 4. Gomez B, Mintegi S, Rubio MC, et al: Clinical and analytical characteristics and short-term evolution of enteroviral meningitis in young infants presenting with fever without source. Pediatr Emerg Care 2012; 28: pp. 518-523 5. Rotbart HA: Diagnosis of enteroviral meningitis with the polymerase chain reaction. J Pediatr 1990; 117: pp. 85-89 6. Sawyer MH, Holland D, and Aintablian N: Diagnosis of enteroviral central nervous system infection by polymerase chain reaction during a large community outbreak. Pediatr Infect Dis J 1994; 13: pp. 177-182 7. Ahmed A, Brito F, Goto C, et al: Clinical utility of polymerase chain reaction for diagnosis of enteroviral meningitis in infancy. J Pediatr 1997; 131: pp. 393-397 8. Shalabi M, and Whitley RJ: Recurrent benign lymphocytic meningitis. Clin Infect Dis 2006; 43: pp. 1194-1197 9. Corey L, and Spear PG: Infections with herpes simplex viruses (2). N Engl J Med 1986; 314: pp. 749-757 10. Kupila L, Vuorinen T, Vainionpaa R, et al: Etiology of aseptic meningitis and encephalitis in an adult population. Neurology 2006; 66: pp. 75-80 11. Tan K, Patel S, Gandhi N, et al: Burden of neuroinfectious diseases on the neurology service in a tertiary care center. Neurology 2008; 71: pp. 1160-1166 12. Glaser CA, Gilliam S, Schnurr D, et al: In search of encephalitis etiologies: diagnostic challenges in the California Encephalitis Project, 1998-2000. Clin Infect Dis 2003; 36: pp. 731-742 13. Tyler KL: Herpes simplex virus infections of the central nervous system: encephalitis and meningitis, including Mollaret’s. Herpes 2004; 11: pp. 57A-64A 14. Raschilas F, Wolff M, Delatour F, et al: Outcome of and prognostic factors for herpes simplex encephalitis in adult patients: results of a multicenter study. Clin Infect Dis 2002; 35: pp. 254-26 15. Domingues RB, Tsanaclis AM, Pannuti CS, et al: Evaluation of the range of clinical presentations of herpes simplex encephalitis by using polymerase chain reaction assay of cerebrospinal fluid samples. Clin Infect Dis 1997; 25: pp. 86-91 16. Whitley RJ, Alford CA, Hirsch MS, et al: Vidarabine versus acyclovir therapy in herpes simplex encephalitis. N Engl J Med 1986; 314: pp. 144-149 17. Lakeman FD, and Whitley RJ: Diagnosis of herpes simplex encephalitis: application of polymerase chain reaction to cerebrospinal fluid from brain-biopsied patients and correlation with disease. National Institute of Allergy and Infectious Diseases Collaborative Antiviral Study Group. J Infect Dis 1995; 171: pp. 857-86 18. Whitley RJ, Alford CA, Hirsch MS, et al: Factors indicative of outcome in a comparative trial of acyclovir and vidarabine for biopsy-proven herpes simplex encephalitis. Infection 1987; 15: pp. S3-S8 19. Kramer LD, Li J, and Shi PY: West Nile virus. Lancet Neurol 2007; 6: pp. 171-181 20. Watson JT, Pertel PE, Jones RC, et al: Clinical characteristics and functional outcomes of West Nile Fever. Ann Intern Med 2004; 141: pp. 360-365 21. Sejvar JJ, Haddad MB, Tierney BC, et al: Neurologic manifestations and outcome of West Nile virus infection. JAMA 2003; 290: pp. 511-515 22. Jean CM, Honarmand S, Louie JK, et al: Risk factors for West Nile virus neuroinvasive disease, California, 2005. Emerg Infect Dis 2007; 13: pp. 1918-1920 23. Shi PY, and Wong SJ: Serologic diagnosis of West Nile virus infection. Expert Rev Mol Diagn 2003; 3: pp. 733-741 24. Garcia MN, Hause AM, Walker CM, et al: Evaluation of prolonged fatigue post-West Nile virus infection and association of fatigue with elevated antiviral and proinflammatory cytokines. Viral Immunol 2014; 27: pp. 327-333 25. Gilden DH, Mahalingam R, Cohrs RJ, et al: Herpesvirus infections of the nervous system. Nat Clin Pract Neurol 2007; 3: pp. 82-94
The ATS and IDSA recently released the much-anticipated update to the community-acquired pneumonia (CAP) guidelines. The previous version was published back in 2007 and the new guidelines have included some major changes. Here is a rundown of all those changes that you need to know.
1. Health care associated pneumonia (HCAP) no longer exists
HCAP was an entity created with the 2007 CAP guidelines. It encompassed non-hospital acquired pneumonia in patients who had recent contact with the healthcare system. The recommendation was to treat HCAP with empiric broad-spectrum antibiotic therapy against methicillin-resistant Staphylococcus aureus (MRSA) and Pseudomonas aeruginosa (PsA). With this strategy however, we were over-treating a lot of people. This study found that while 30% of all patients hospitalized for CAP received empiric anti-MRSA treatment, only 0.7% of all patients had MRSA pneumonia.
In the new guidelines, HCAP no longer exists. Instead, the guidelines emphasize assessment of risk factors for pathogens such as MRSA and PsA.
2.Treatment is now based on severity of the pneumonia rather than the location of the admitted patient
Prior guidelines differentiated antibiotic recommendations based on patient triage to the floor or the intensive care unit. In the new guidelines, treatment recommendations are based on the severity of the pneumonia, based on a list of criteria:
3.Only obtain blood cultures in severe CAP or if risk factors for MRSA and/or PsA are present
The new guidelines focus on cost-effective use of diagnostic tests. Outpatient setting: recommend against any diagnostic testing (except for a chest X-ray) Inpatient non-severe pneumonia: recommend blood cultures and sputum gram stain/culture ONLY if risk factors for MRSA and/or PsA are present Inpatient severe pneumonia: recommend blood cultures, sputum gram stain/culture, Streptococcus pneumoniae urine antigen, and Legionella urine antigen and PCR/culture *Legionella diagnostic tests are also recommended in times of an outbreak
These recommendations are based on literature demonstrating that:
Overall prevalence of true positive blood cultures is 1-9% in patients with CAP3-6
The majority of true positive blood cultures occur in patients with severe CAP6,7
Blood culture results change clinical management in <2% of patients with CAP3,4,6
The rate of blood culture contaminants is similar to the rate of true blood culture positives, resulting in unnecessary antibiotics and extended lengths of stay in the hospital3,4,6
4. Procalcitonin should NOT be used in the diagnosis of CAP
Procalcitonin is not a reliable marker for diagnosis of bacterial infections; it has roughly 65-75% sensitivity for detecting bacterial pneumonia8. Consequently, the risk of not treating bacterial CAP due to a low procalcitonin level can lead to poor outcomes. Although there is data to support use of procalcitonin in determining the duration of antibiotics in CAP9,10, the guidelines recommend use only in situations where duration exceeds the recommended 5-7 days.
The argument from the guideline authors is that there is more literature in support for PSI in accurately predicting mortality rather than the CURB-65 score11-14. However, PSI incorporates data that may not be available in all circumstances, and certainly will not be available to the outpatient clinician who is trying to decide whether to admit a patient or not (such as pH, which can only be obtained from an arterial blood gas). So, although PSI may be recommended for use in the emergency department, the CURB-65 will likely remain in use, especially due to its efficiency in the outpatient setting.
6.Algorithm for CAP antibiotic treatment The meat of the guidelines is the treatment regimens – and there are quite a few changes.
1) Macrolides are no longer recommended as first line therapy in uncomplicated outpatient CAP unless the local streptococcal resistance to azithromycin is <25% (this study shows that most parts of the U.S. have resistance rates >25%).
2) Amoxicillin and doxycycline take the place of macrolides as first line treatment in uncomplicated outpatient CAP.
You may be thinking – “wait, amoxicillin doesn’t even cover atypical pathogens (i.e. Mycoplasma pneumoniae and Legionella pneumophila)!” This is true. But studies have shown that in otherwise-healthy patients, there was no difference in outcomes among those who received amoxicillin vs. an antibiotic that treats atypical organisms16. Exactly why that is remains unclear, but could be because healthy individuals clear the infection on their own or because the majority of these pneumonias are actually due to a virus, so they would improve with or without any antibiotics 5.
3) In hospitalized patients:
Non-severe CAP – only treat empirically for MRSA and/or PsA if the organism has been isolated from the patient’s respiratory tract in the past
Severe CAP – treat empirically for MRSA and/or PsA if the patient has any risk factors for MRSA and/or PsA respiratory infection
7.Treat anaerobes only in cases with suspected or proven lung abscess and/or empyema
Empiric treatment of anaerobes in aspiration pneumonia remains controversial, but the new guidelines recommend only treating anaerobes if there is suspicion for or a proven lung abscess and/or empyema.
8.Continue antibiotics for at least 48 hours in patients who are diagnosed with influenza pneumonia
This recommendation is based off the data that influenza infection predisposes to subsequent bacterial superinfections17 and a patient could have both a viral and a bacterial pneumonia at the same time. The guidelines state that if there is significant clinical improvement in 48 hours and no evidence to suggest a superimposed bacterial pneumonia, antibiotics can be discontinued at that time.
9. Duration of antibiotics is based on clinical improvement (but should be a minimum of 5 days)
Gone are the days of prespecified number of days for antibiotic duration. Instead, monitor the patient for signs of clinical improvement.
If cultures are not growing MRSA and/or PsA, can stop empiric treatment for MRSA and/or PsA.
If clinically improving, stop antibiotics following 48 hours of clinical improvement after a minimum of 5 days. Clinical improvement is determined by resolution of vital sign abnormalities, ability to eat/improved appetite, and normal mentation.
10. Do not use corticosteroids as adjunctive treatment and do not obtain routine follow up chest X-rays
These were not necessarily strategies that I employed prior to the publication of these guidelines, and corticosteroid use in CAP is controversial, but at this time, there is no strong data to support either of these adjunctive management strategies in patients with CAP.
References:
1. Metlay JP, Waterer GW, Long AC, et al. Diagnosis and Treatment of Adults with Community-acquired Pneumonia. An Official Clinical Practice Guideline of the American Thoracic Society and Infectious Diseases Society of America. Am J Resp Crit Care Med. 2019; 200(7):e45-e67. 2. Self WH, Wunderink RG, Williams DJ, et al. Staphylococcus aureus Community-acquired Pneumonia: Prevalence, Clinical Characteristics, and Outcomes. Clin Infect Dis. 2016; 63(3):300-309. 3. Chalasani NP, Valdecanas MA, Gopal AK, McGowan JE Jr, and Jurado RL. Clinical utility of blood cultures in adult patients with community-acquired pneumonia without defined underlying risks. Chest. 1995; 108(4):932-936. 4. Corbo J, Friedman B, Bijur P, and Gallagher EJ. Limited usefulness of initial blood cultures in community acquired pneumonia. Emerg Med J. 2004; 21(4):446-448. 5. Jain S, Self WH, Wunderink RG, et al. Community-Acquired Pneumonia Requiring Hospitalization among U.S. Adults. New Eng J Med. 2015. 373:415-427. 6. Lee JH and Kim YH. Predictive factors of true bacteremia and the clinical utility of blood cultures as a prognostic tool in patients with community-onset pneumonia. Medicine (Baltimore). 2016; 95(41):e5058. 7. Waterer GW and Wunderink RG. The influence of the severity of community-acquired pneumonia on the usefulness of blood cultures. Respir Med. 2001; 95(1):78-82. 8. Self WH, Balk RA, Grijalva CG, et al. Procalcitonin as a Marker of Etiology in Adults Hospitalized With Community-Acquired Pneumonia. Clin Infect Dis. 2017;65(2):183-190. 9. Schuetz P, Wirz Y, Sager R, et al. Procalcitonin to initiate or discontinue antibiotics in acute respiratory tract infections. Cochrane Database Syst Rev. 2017; 10:CD007498. 10. Schuetz P, Wirz Y, Sager R, et al. Effect of procalcitonin-guided antibiotic treatment on mortality in acute respiratory infections: a patient level meta-analysis. Lancet Infect Dis. 2018;18(1):95-107. 11. Aujesky D, Auble TE, Yealy DM, et al. Prospective comparison of three validated prediction rules for prognosis in community-acquired pneumonia. Am J Med. 2005; 118(4):384-392. 12. Marrie TJ, Lau CY, Wheeler SL, Wong CJ, Vandervoort MK, and Feagan BG. A controlled trial of a critical pathway for treatment of community-acquired pneumonia. CAPITAL Study Investigators. Community-Acquired Pneumonia Intervention Trial Assessing Levofloxacin. JAMA. 2000; 283(6):749-755. 13. Carratala J, Fernandez-Sabe N, Ortega L, et al. Outpatient care compared with hospitalization for community-acquired pneumonia: a randomized trial in low-risk patients. Ann Intern Med. 2005;142(3):165-172. 14. Renaud B, Coma E, Labarere J, et al. Routine use of the Pneumonia Severity Index for guiding the site-of-treatment decision of patients with pneumonia in the emergency department: a multicenter, prospective, observational, controlled cohort study. Clin Infect Dis. 2007;441(1):41-49. 15. Blondeau JM and Theriault N. Application of the Formula for Rational Antimicrobial Therapy (FRAT) to Community-Acquired Pneumonia. J Infect Dis Ther. 2017;5:313. 16. Postma DW, van Werkhoven CH, van Elden LJR, et al. Antibiotic Treatment Strategies for Community-acquired Pneumonia in Adults. New Eng J Med. 2015;372:1312-1323. 17. Metersky ML, Masterton RG, Lode H, File TM Jr, and Babinchak T. Epidemiology, microbiology, and treatment considerations for bacterial pneumonia complicating influenza. Int J Infect Dis. 2012;16(5):e321-331.
HIV infection has changed dramatically over the last few decades. When we admit patients with HIV to the hospital, the way to approach them can vary widely depending on their immune status and how well their virus is controlled.
In this post, I present a series of steps that you should think about when admitting a patient with HIV to the hospital.
1. ADDRESS privacy concern
Even in 2019, there is significant stigma and discrimination surrounding HIV and those people who live with HIV (PLWH)1. Thus, it’s very important that their HIV status is not disclosed to others without the patient’s permission.
If there are other non-healthcare personnel in the room with the patient (i.e. family members, friends, other patients within hearing distance), do not mention their HIV status until confirmed by patient that it is permissible to discuss it in front of the other individuals.
Options for opening the discussion:
A) “Is it okay if I discuss all your medical conditions in front of these individuals or would you rather talk in private”?
B) Ask everyone else to leave – this will allow you to ask about HIV as well as other potentially sensitive subjects such as sexual history and domestic violence.
C) Proceed with the H&P and ask the patient about their medical history – observe whether they mention HIV or not. If they do not, then do not mention it and come back at a later time to speak to them privately or ask the guests to leave the room for the exam and ask about HIV at that time.
D) If the patient is sharing the room with another patient, then I usually ask about their “viral infection”. Almost all PLWH will know what you are referring to. Then I wait to see if the patient mentions the word “HIV” or “AIDS” themselves – if they do, then I take that as a signal that it is permissible to talk about it openly (in that particular setting only) and if they do not, then I proceed with as much information as I can elicit without using the word “HIV” or making it obvious that I am discussing “HIV”.
2. ASSESS the immune status
The immune status is determined by their CD4+ count/percentage. However, usually you don’t know their current CD4+ count at the time of admission. What to do?
a) If they have been to your hospital/system before, check their chart for prior CD4+ counts. That should give you a general idea of their immune status. –if patient is taking antiretroviral therapy (ART), current CD4+ is likely the same or improved –if patient stopped/not taking ART, current CD4+ is likely the same or worsened
b) Ask the patient! Most of the patients know their CD4+ counts or at least know if its low or high
*Also, please keep in mind that CD4+ counts are affected by changes in total white blood cell counts, so in an acute illness, the CD4+ percentage (which is not affected by the WBC count) is a more stable marker of immune status. Generally, a CD4+ count obtained during a routine office visit will be more accurate of their immune status than one obtained during a hospital admission.3
3. DEVELOP differential for their concern/symptoms based on immune status
A. If CD4+ >500cells/mm3, then their immune system is intact and there is low likelihood of opportunistic infections.
B. If CD4+ 200-500cells/mm3, then their immune system remains compromised and still susceptible to infections. Also, there is potential that since the last CD4+ count, they have stopped taking their medications and could now be below 200cells/mm3. Consider opportunistic infections, but should be lower on the differential.
C. If CD4+ <200cells/mm3, opportunistic infections NEED to be on your differential. Treat the patient as an immunocompromised individual and tailor empiric therapy as appropriate.4,5,6
*However, common things being common — a patient with HIV is still at risk for other non-opportunistic infections such as bacterial pneumonia and hospital-acquired infections.
4. FIND OUT if they are currently taking ART and which ones?
A.If
they are not taking ART, then do not start ART on admission until discussed
with an HIV provider
B.If
patient has ART prescribed but has not been taking them, do not restart the
medications on admission until discussed with the patient’s HIV provider.
Starts and stops in the medications can promote viral resistance to the drugs.
C.If patient is on ART, continue the ART (unless clear obvious reason not to, i.e. allergy). Find out from patient, family member (who is aware of status), HIV provider/PCP, pharmacy, or medical record what treatment they are on – often patients will be on a combination pill that may not be available in your hospital. In these cases, look up the individual medications in the combination pill and prescribe them all separately.7
5. RUN a
drug interaction check when starting ANY new medications
Failure to do this can cause increased metabolism of the HIV medications leading to resistance, or cause increased/decreased metabolism of the other medications leading to inadequate treatment or toxicity. Use this website to check for drug-drug interactions.
6. DETERMINE most recent HIV viral load
–if patient has been on ART regularly, then viral load will likely be undetectable –if patient has not been on ART regularly, then viral load will likely be detectable
7. TAKE a sexual history
– assess risk for other STDs – assess risk for HIV transmission to sexual partners – educate on U=U and PrEP
8. ASK them about their experience and history of HIV, once you to get to know them.
You will learn a lot that medical books will never be able to teach you.
Was this helpful? Did I miss something? Let me know in the comments!
References 1. Turan B, Budhwani H, Fazeli PL, Browning WR, Raper JL, Mugavero MJ, et al. How Does Stigma Affect People Living with HIV? The Mediating Roles of Internalized and Anticipated HIV Stigma in the Effects of Perceived Community Stigma on Health and Psychosocial Outcomes.AIDS Beh. 2017; 21(1):283-291. 10.1007/s10461-016-1451-5. 2. Shapiro NI, Karras DJ, Leech SH, and Heilpern KL. Absolute lymphocyte count as a predictor of CD4 count. Ann Emerg Med. 1998; 32(3 Pt 1):323-328. 10.1016/s0196-0644(98)70008-3 3.Feeney C, Bryzman S, Kong L, Brazil H, Deutsch R, and Fritz LC. T-lymphocyte subsets in acute illness. Crit Care Med. 1995; 23(10):1680-1685. 10.1097/00003246-199510000-00012 4. Taylor JM, Sy JP, Visccher B, and Giorgi JV. CD4+ T-cell number at the time of acquired immunodeficiency syndrome.Am J Epidemiol. 1995; 141(7): 645-651. 10.1093/oxfordjournals.aje.a117480 5. Hanson DL, Chu SY, Farizo KM, and Ward JW. Distribution of CD4+ T lymphocytes at diagnosis of acquired immunodeficiency syndrome-defining and other human immunodeficiency virus-related illnesses. The Adult and Adolescent Spectrum of HIV Disease Project Group.Arch Intern Med. 1995; 155(14):1537-1542. 6. Mocroft A, Furrer HJ, Miro JM, Reiss P, Mussini C, Kirk O, et al. The incidence of AIDS-defining illnesses at a current CD4 count ≥ 200 cells/μL in the post-combination antiretroviral therapy era. Clin Infect Dis. 2013; 57(7):1038-1047. 10.1093/cid/cit423 7. Management of the Treatment-Experienced Patient. AIDSInfo. Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents with HIV. U.S. Department of Health and Human Services. Site updated August 29, 2019. Retrieved August 29, 2019. https://aidsinfo.nih.gov/guidelines/html/1/adult-and-adolescent-arv/18/discontinuation-or-interruption-of-antiretroviral-therapy10.1097/00003246-199510000-00012
When I was an aspiring Infectious Disease fellow, I marveled at how the ID doctors would come up with diseases that no one else had thought of. How did they do that?
They obtain a detailed patient history. (It’s the ID doctors equivalent of a procedure!)
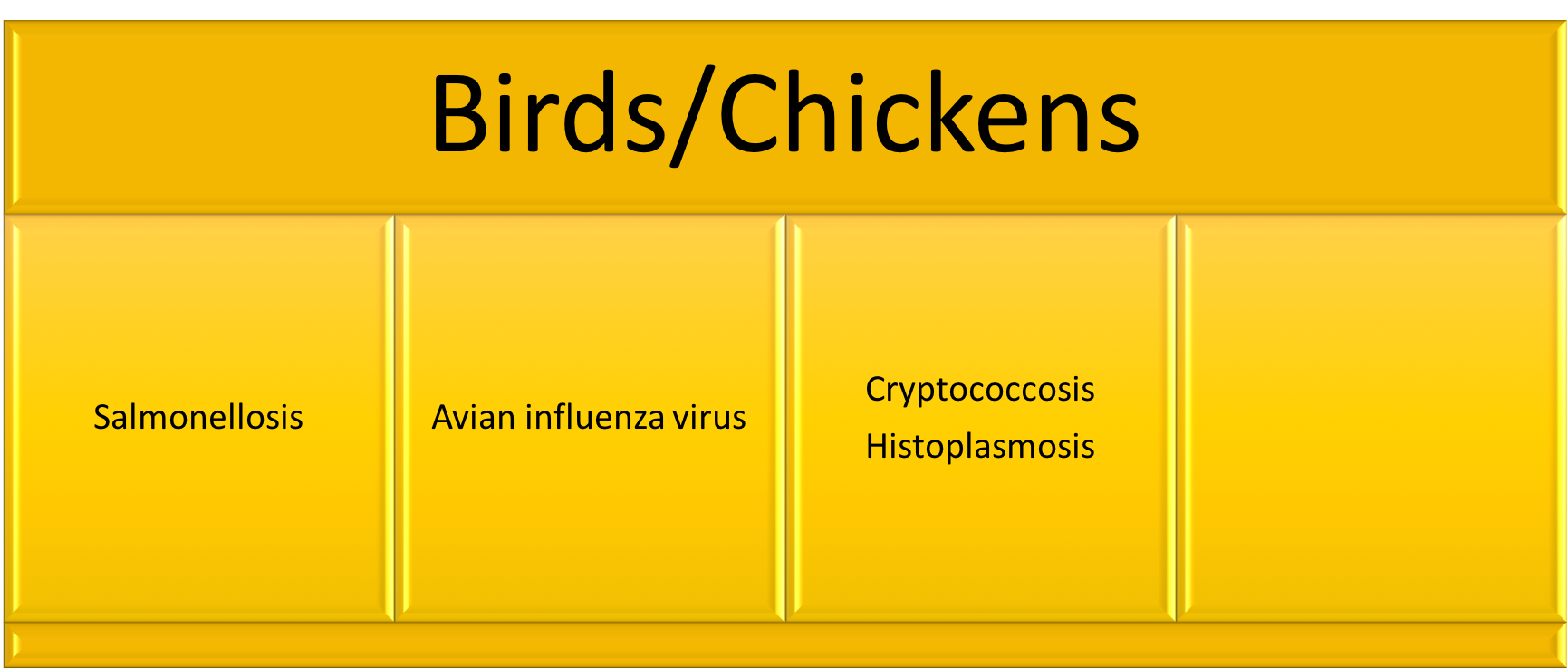
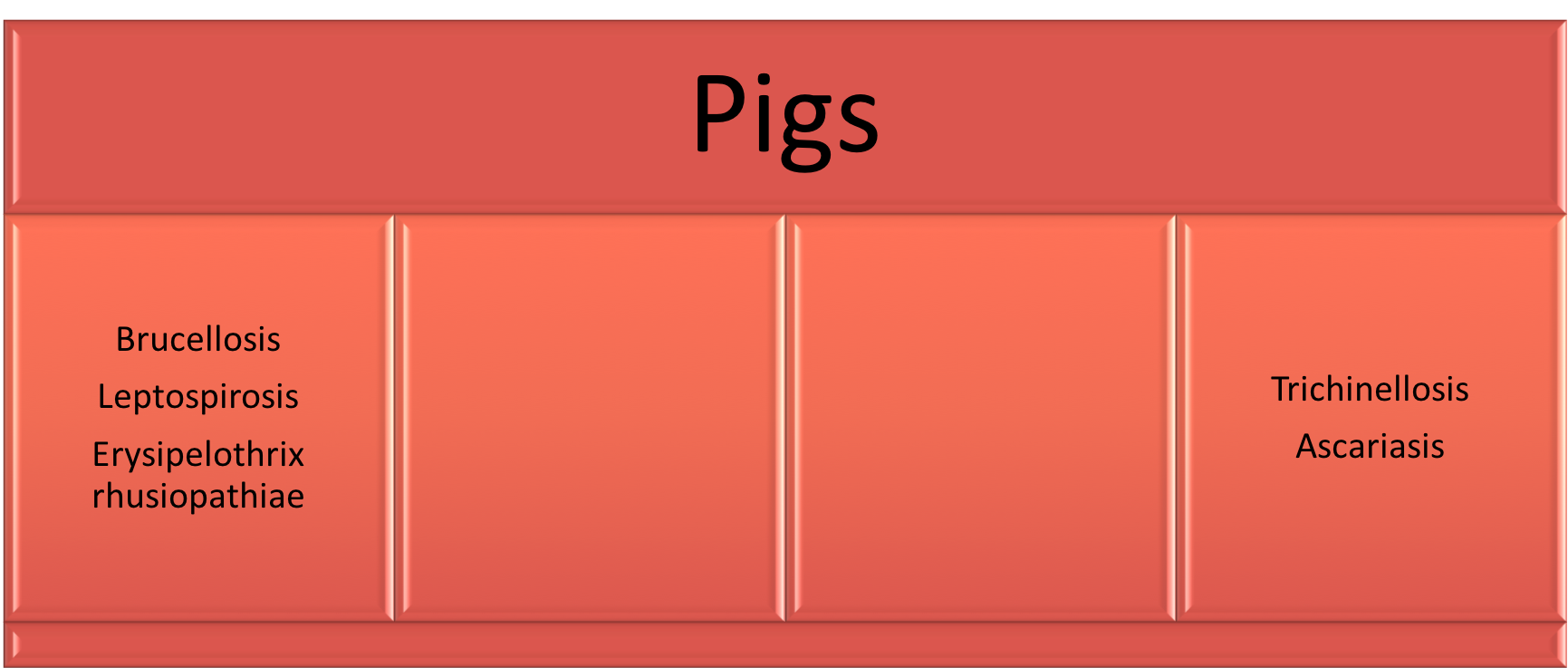
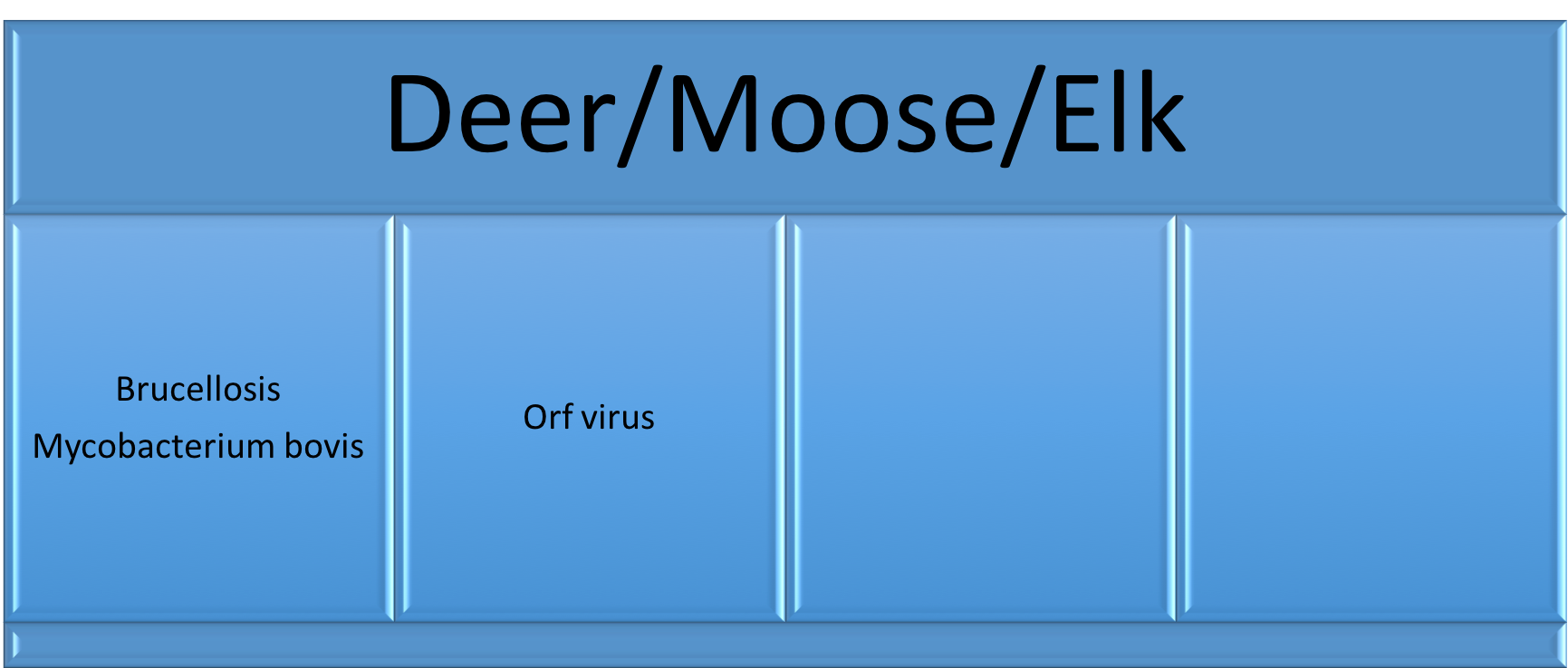
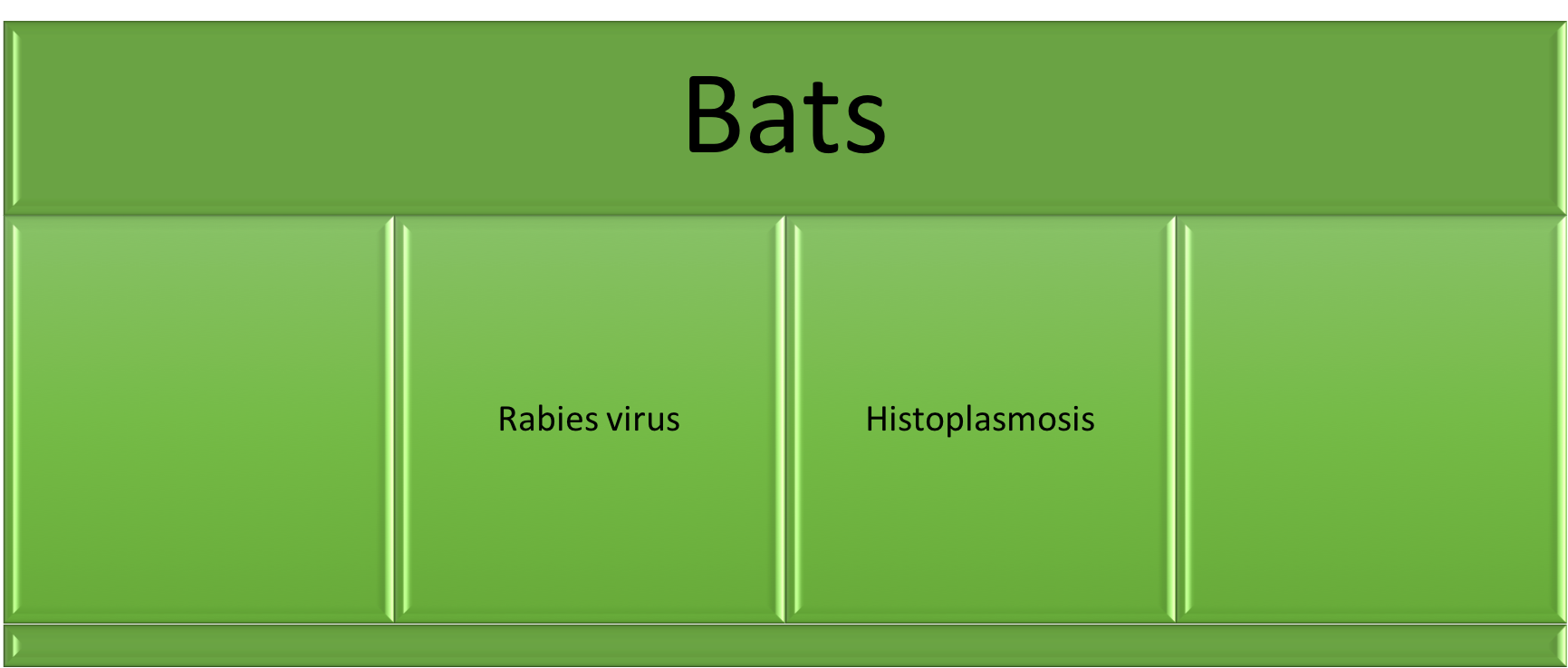
Contact or exposure to certain animals are associated with certain diseases.
These are examples of some of the questions to ask to ascertain whether your patient has been in contact with specific animals: – Do you have any pets? Do you have frequent contact with anyone else’s pets? – Do you have contact with any farm or wild animals? – What do you do for work (farmer, veterinarian, kennel worker, biologists, etc)? – What do you do for fun (hunting, fishing, cave explorer, raising chickens, etc)?
I’ve created an easy graphic to give you an idea of some diseases that are associated with different animals your patients might encounter. This is to help you quickly look up which infections you should consider in your differential if your patient reports an exposure to one of these animals.
*This list does not include ALL pathogens. This is just a list of the most common plus others to think about in certain situations. In places outside of North America, this list may look different. **This is not intended to take the place of a formal infectious disease consult. ***Use this chart in the context of the clinical presentation. It does not mean you should test for all these infections in every patient, but rather gives you a quick reminder to consider them in your differential.
Was this helpful? Did I miss something? Tell me what you’re thinking with a comment!
References:
1. Centers for Disease Control and Prevention. Healthy Pets Healthy People. http://www.cdc.gov/healthypets/pets/cats.html (Accessed on Feb 23, 2019). 2. Day MJ. Pet-Related Infections. Am Fam Physician. 2016; 94(10):794-802. 3. Goldstein EJC and Abrahamian FM. Diseases Transmitted by Cats. Microbiol Spectr. 2015; 3(5). 4. Chomel BB. Emerging and Re-emerging Zoonoses of Dogs and Cats. Animals (Basel). 2014; 4(3):434-445. 5. Dyer JL, Yager P, Orciari L et al. Rabies surveillance in the United States during 2013. J Am Vet Med Assoc. 2014; 245(10):1111-1123. 6. Boseret G, Losson B, Mainil JG, et al. Zoonoses in pet birds: review and perspectives. Vet Res. 2013; 44(1): 36. 7. Kwon-Chung KJ, Fraser JA, Doering TL, et al. Cryptococcus neoformans and Cryptococcus gattii, the Etiologic Agents of Cryptococcosis. Cold Spring Harb Perspect Med. 2014; 4(7):a019760. 8. National Association of State Public Health Veterinarians, Inc. (NASPHV), Centers for Disease Control and Prevention (CDC). Compendium of measures to prevent disease associated with animals in public settings, 2011: National Association of State Public Health Veterinarians, Inc. MMWR Recomm Rep 2011; 60:1. 9. Kotton CN. Zoonoses from pets other than dogs and cats. UpToDate. Published Jan 2019. Accessed on Feb 23, 2019.
Tuberculosis is the leading cause of death globally from an infectious agent. In 2017, an estimated 10 million people developed TB disease and an estimated 1.6 million died1. A recent study demonstrated that <57% of internal medicine housestaff across 7 academic institutions in the U.S. correctly answered 9 out of 10 questions assessing knowledge of assessment and diagnosis of tuberculosis2. This post addresses these questions and to helps clarify latent vs. active TB in a clinical setting.
The primary focus for this blog post is pulmonary TB. Be aware that although the most common presentation of TB is with pulmonary symptoms, TB can present anywhere in the body and sometimes can present without pulmonary symptoms.
But first, definitions.
Definitions
Latent infection – the bacteria lies dormant in the body and does not cause any symptoms, typically tests for latent infection (see later section) will be positive
Active disease – the individual is experiencing symptoms due to the infection in the body, typically with characteristic imaging findings and microbiological confirmation
Primary disease – immediate onset of active disease after infection
Reactivation disease – onset of active disease after a period of latent infection
Extra-pulmonary disease – presence of bacteria outside of the lungs (the primary organ of infection)
Disseminated disease – two or more noncontiguous sites resulting from lymphohematogenous dissemination
Miliary disease – lesions in the lung that resemble millet seeds; seen in some cases of disseminated TB
Step 1: Risk stratification
Risk factors for TB exposure
having close contact with individuals who have active tuberculosis (roommates, family, friends, caregivers)
living/had lived in a country that is endemic for TB
living/working in a prison
living/working in a homeless shelter
injecting drugs
living/working in any other facility/institution that has high rate of TB (hospitals, nursing homes, residential homes for HIV patients)
*USPSTF gives a grade B recommendation for screening those at increased risk (see list above) for latent tuberculosis infection4
Risk factors for TB reactivation
A. Normal host
5-10% of reactivating TB in a lifetime6,13
50% of that 5-10% is within the first 2-5 years of infection6,13
B. Age – immunity weakens in the elderly
C. Immunosuppression
HIV
End stage renal disease
Diabetes mellitus
Lymphoma
Corticosteroid or TNF-alpha inhibitor use
Cigarette smoking
Step 2: Why is it important to distinguish latent TB from active TB?
The two syndromes are treated completely differently. Latent TB is non-infectious and does not require treatment to prevent progression of disease or transmission to others, but instead to prevent future reactivation. Active TB is infectious and needs to be treated to prevent spread of TB to others. The medications, doses and duration of therapy to treat these syndromes are also different from each other.
Active TB
A. Clinical symptoms
fevers/chills, night sweats, weight loss, SOB and/or cough
depending on site of TB disease, can have extrapulmonary symptoms (GI, CNS, spine, etc)
subacute to chronic onset of symptoms (typically > several weeks)
B. Imaging
will typically have active pulmonary abnormalities seen on imaging (this can be any type of abnormality – infiltrates, cavitary lesions, effusions, or solitary nodules)
although the most common cause of apical lung scarring is prior TB infection, lung abnormalities DO NOT have to be in the apices of the lungs (they can be anywhere)
Latent TB (make diagnosis ONLY after you have excluded active TB)
A. Clinical symptoms
the patient is asymptomatic (= NO symptoms of active TB)
B. Imaging
there is no active lung abnormality on chest imaging
(calcified granulomas/nodules or anything that is deemed old, healed scarring is excluded)
*If there are any signs suggestive of active TB, then the patient should undergo active TB evaluation (discussed below). If there is no evidence of active TB, then treatment can be based on latent TB diagnostics (discussed below).
Step 3: Evaluating for TB – diagnostic tests
A. Active TB tests (pulmonary TB)
obtain 2-3 sputum samples, ideally at least 8 hours apart, may require sputum induction if patient is not able to cough up sputum.
one ideally should be in the morning (highest burden of TB in the morning due to pooling of secretions overnight)
obtaining a bronchoscopy sample only counts for one sample
send a nucleic acid amplification test (NAAT) on the 1st sputum sample
1. AFB smear – fluorochrome stain of the clinical specimen
sensitivity = 67.5% (95% CI, 60.6 to 73.9)8
specificity = 97.5% (95% CI, 97.0 to 97.9)8
2. AFB culture – the gold standard test for tuberculosis diagnosis
can take up to 6 weeks to grow for solid culture versus ~ 2 weeks for liquid culture
3. PCR = NAAT (nucleic acid amplification test) – this is a DNA test using amplification methods
GeneXpert MTB/RIF assay is a brand test that combines the NAAT with rapid test for rifampin resistance sensitivity and specificity are high in pulmonary tuberculosis but is lower when used on specimens other than sputum.
sensitivity: 98% (for smear-positive, culture-positive specimens in HIV-negative patients)9
specificity: 99%9
this test can be run on both AFB smear negative and positive specimens (although sensitivity is lower on AFB smear negative specimens)
more specific than the smear because it tests directly for tuberculosis genes, whereas positive AFB smears can be due to non-tuberculous mycobacteria or other acid-fast staining bacteria (i.e. Nocardia)
positive result → TB diagnosis negative result → does not rule out TB
B. Latent TB tests
1. Tuberculin Skin Test (TST) = Purified Protein Derivative (PPD)
intradermal injection of tuberculin material (many different materials available)
causes a delayed-type hypersensitivity response in individuals whose immune system has been exposed to TB before
positive test = induration at the injection site within 48-72 hours
negative test = no induration
Threshold for treatment
TB, tuberculosis; CXR, chest X-ray; HIV, human immunodeficiency virus; IBW, ideal body weight
*individuals who have received the BCG vaccine in the past may also test positive with this test since their immune systems have been exposed to TB via the vaccine (although immunity tends to wane within 10 years if vaccine is administered in infancy)
2. Interferon Gamma Release Assay (IGRA) = QuantiFERON-TB Gold or Plus OR T-SPOT.TB
blood test for detection of cell-mediated immune response to TB antigen
not affected by BCG vaccine or BCG treatment
80-90% sensitivity, >95% specificity (sensitivity is diminished in immunocompromised hosts)5
the QuantiFERON-TB Gold test is made up of 3 tubes:
negative control (everyone should not react)
positive control (everyone should react), and the
TB antigen that is recognized by CD4 cells
**QuantGold-PLUS (a new test) has added a 4th tube with TB antigen that binds to CD8 cells thereby increasing sensitivity of the test12
positive test → patient’s blood reacted to the TB antigen and positive control but not the negative control
negative test → patient’s blood did not react to the TB antigen but did react to the positive control
indeterminate test → patient’s blood did not react to the positive control so test is invalid (this typically happens when the patient is immunocompromised and cannot mount an immune response to the positive control and thus would not react to the TB antigen either – even if they were exposed to TB)
*Indeterminate result DOES NOT mean it is in the middle between negative and positive. It means the test cannot provide a valid result.
*all latent diagnostic tests can cross-react in individuals infected with non-tuberculous mycobacteria (TST more so than the IGRA)
*Neither test is 100% sensitive and specific – if the patient has high pre-test probability for TB exposure and for future TB reactivation, ID physicians will sometimes treat for latent TB despite the negative tests
Step 4: Treating TB
Treatment is complex and both choice of medication and duration depends on a variety of clinical and microbiological factors. Here is a basic overview of the difference in treatment between latent and active TB.
A. Latent TB (CDC)
*This is a useful calculator to determine the risks and benefits of TB reactivation vs. side effects from treatment in an individual patient.
a) Isoniazid – daily for 6 to 9 months
b) Rifampin – daily for 4 months
c) Rifapentine and isoniazid – weekly for 3 months
B. Active TB — depends on susceptibility of bacteria and clinical syndrome — RIPE therapy is the standard first-line therapy for fully-susceptible pulmonary TB infection with 2 months of all four drugs followed by 4 months of rifampin and isoniazid.
R = rifampin
I = isoniazid
P = pyrazinamide
E = ethambutol
*Ethambutol can be discontinued if drug susceptibility testing confirms a fully susceptible strain
*Patients with extensive disease e.g. cavitation or who remain smear and/or culture positive at 2 months may require a longer duration of therapy.
Don’t forget to:
give daily Vitamin B6 with isoniazid to prevent peripheral neuropathy
get baseline eye exam when starting ethambutol to enable monitoring for optic neuritis, particularly in patients with abnormal renal function
evaluate for other co-morbidities such as HIV, hepatitis B or C, diabetes or substance use
References:
1. Global Tuberculosis Report 2018: Executive Summary. World Health Organization. Published Sept 2018. Accessed Mar 10, 201
2. Chida N, Brown C, Mathad J, et al. Internal Medicine Residents’ Knowlesge and Practice of Pulmonary Tuberculosis Diagnosis. OFID. 2018; 5(7).
3. Tuberculosis (TB). Centers for Disease Control and Prevention. Available from: https://www.cdc.gov/tb. Accessed Feb 13, 2019.
4. US Preventive Services Task Force. Screening for Latent Tuberculosis Infection in Adults. US Preventive Services Task Force Recommendation Statement. JAMA. 2016; 316(9):962-969. doi:10.1001/jama.2016.11046
5. Lewinsohn DM, Leonard MK, LoBue PA, et al. Official American Thoracic Society/Infectious Disease Society of America/Centers for Disease Control and Prevention Clinical Practice Guidelines: Diagnosis of Tuberculosis in Adults and Children. Clin Infect Dis. 2017; 64(2):111-115. doi: 10.1093/cid/ciw778
6. Horsburgh CR. Priorities for the Treatment of Latent Tuberculosis Infection in the United States. N Engl J Med. 2004; 350:2060-2067. DOI: 10.1056/NEJMsa031667
7. Pai M, Behr MA, Dowdy D, et al. Primer: Tuberculosis. Nature Reviews. 2016; 2:1-23.
8. Mathew P, Yen-Hong K, Vazirani B, Eng RHK, and Weinstein MP. Are Three Sputum Acid-Fast Bacillus Smears Necessary for Discontinuing Tuberculosis Isolation? J Clin Microbiol. 2002; 40(9):3482-3484. doi: 10.1128/JCM.40.9.3482-3484.2002
9. Steingart KR, Schiller I, Horne DJ, Pai M, Boehme CC, and Dendukuri N. Xpert® MTB/RIF assay for pulmonary tuberculosis and rifampicin resistance in adults. Cochrane Database Syst Rev. 2014 Jan 21;(1):CD009593. doi: 10.1002/14651858.CD009593.pub3.
10. Zeka AN, Tasbakan S, and Cavusoglu C. Evaluation of the GeneXpert MTB/RIF Assay for Rapid Diagnosis of Tuberculosis and Detection of Rifampin Resistance in Pulmonary and Extrapulmonary Specimens. 2011; 49(12):4138-4141. doi:10.1128/JCM.05434-11.
This post is co-written with the guest writer Ahmed Abdul Azim, MD.
Not all fevers are caused by infections.
It is important that every patient presenting with fever is evaluated for an infection….. but what do you do when no infection is found?
Why are non-infectious causes of fever important to know?
If a patient is treated for a presumed infectious fever when they don’t have an infection:
there is a delay in identifying the correct diagnosis
they are exposed to prolonged courses of unnecessary antibiotics
Definition of fever
Fever = 38.3°C (101°F) or above1
Pyrogenic agents = substances that can induce a fever.
a) Exogenous pyrogens – external substances that activate our immune system to induce a fever (ex. microbial toxins)
b) Endogenous pyrogens – cytokines that induce fever in our body
(ex. IL-1, IL-6, tumor necrosis factor, IFN-α, ciliary neutrotrophic factor, and likely others)
Non-infectious causes of fever:
1. Rheumatologic/autoimmune – activation of immune system that stimulates the production of pyrogenic cytokines
– the cause of ~30% of fevers of unknown origin
a) Adult-onset Still’s disease – younger patients, daily fevers >39°C, rash, arthritis
b) Giant cell arteritis – older patients, vision changes, jaw claudication
c) Others – polyarteritis nodosa, Takayasu’s arteritis, granulomatosis with polyangiitis, etc.
a) Lymphomas and leukemias – most common; seen in high burden of disease
b) Myelodysplastic syndromes
c) Renal cell carcinoma – ~20% of cases present with fevers
d) Hepatocellular carcinoma or liver metastases
e) Atrial myxomas
3. Drug-induced fever – 3-5% of drug-related adverse reaction in hospitalized patients include fevers6 – typically occurs 7-10 days after drug initiation, but can be as soon as 24 hours and as far away as a few years from drug initiation7 – patients typically appear “inappropriately” well
– eosinophilia (>500/mm3) occurs in 20-25% of patients with drug-induced fevers10 – PATHOPHYSIOLOGY:
a) Hypersensitivity reaction – due to activation of T cell immune response by drug, its metabolite, or the formation of an immune complex
– typically occurs ~3-10 days after drug exposure
– typically resolves 72-96 hours after discontinuation of drug (but can be more delayed)
– symptoms will recur immediately upon rechallenge
1) Antimicrobials – most common cause of drug fever
– minocycline, beta-lactams (penicillin-based > cephalosporins10), sulfonamides, nitrofurantoin
2) Anticonvulsants – carbamazepine, phenytoin, phenobarbital
3) Allopurinol
4) Others
– DRESS syndrome – a severe type of drug hypersensitivity reaction
(typically occurs 2-6 weeks after drug exposure)
b) Administration-related – typically last <48 hours
1) Vaccines – stimulation of the immune system → release of pyrogenic cytokines
2) Amphotericin B – exogenous pyrogenic agents
c) Pharmacologic action of the drug– transient fever; self-resolving
1) Anti-neoplastic agents – cause severe and rapid tumor cell lysis → release of endogenous pyrogenic agents → inflammatory response (fever)
2) Antimicrobials – cause rapid death of microbes → microbial cell lysis → release of exogenous pyrogenic substances → inflammatory response (fever)
– ex. Jarisch-Herxeimer reaction in syphilis treatment with penicillin
d) Altered thermoregulation – disturbance of the central hypothalamic thermoregulation function and/or increased heat production
1) Transfusion of blood cells – RBCs, platelets, WBCs
2) Central fevers – fevers due to central thermodysregulation due to CNS damage
– more common with CNS hemorrhage and brain tumors11 – fever onset within 72 hours of sustaining CNS hemorrhage
3) Thromboembolism – typically <102°F
4) Endocrine – thyroid storm; adrenal insufficiency
5) Pulmonary – ARDS, aspiration pneumonitis, cryptogenic organizing pneumonia
6) Intra-abdominal – acute pancreatitis, cholecystitis, mesenteric ischemia
*Non-infectious causes of fevers are diagnoses of exclusion. A patient MUST have an appropriate workup for infectious causes prior to considering any of the non-infectious causes of fever.
*A lot of these diagnoses need to be made based on clinical symptoms and signs and requires a high degree of suspicion.
*Fever is a sign of an underlying inflammatory process. DO NOT TREAT THE FEVER — TREAT THE UNDERLYING CAUSE.
References:
O’Grady NP, Barie PS, Bartlett JG, et al. Guidelines for evaluation of new fever in critically ill adult patients: 2008 update from the American College of Critical Care Medicine and the Infectious Diseases Society of America. Crit Care Med. 2008; 36(4):1330-1349.
Dekker AR, Verheij TJ, and van der Velden AW. Inappropriate Antibiotic Prescription for Respiratory Tract Indications: Most Prominent in Adult Patients. Family Practice. 2015; 32(4):401-407.
Mackowiak PA, Wasserman SS, and Levine MM. A Critical Appraisal of 98.6°F, the Upper Limit of the Normal Body Temperature, and Other Legacies of Carl Reinhold August Wunderlich. JAMA. 1992; 268(12):1578-1580.
Obermeyer Z, Samra JK, and Mullainathan S. Individual Differences in Normal Body Temperature: Longitudinal Big Data Analysis of Patient Records. BMJ. 2017; 359:j5468.
Westbrook A, Pettila V, Nichol A, et al. Transfusion Practice and Guidelines in Australian and New Zealand Intensive Care Units. Intensive Care Med. 2010; 36(7):1138-1146.
Lipsky, BA and Hirschmann JV. Drug Fever. JAMA. 1981; 245(8):851-854.
Mackowiak, PA. Southwestern Internal Medicine Conference: Drug Fever: Mechanisms, Maxims and Misconceptions. Am J Med Sci. 1987; 294(4):275-286.
Patel, RA and Gallagher JC. Drug fever. Pharmacotherapy. 2010; 30(1):57-69.
Johnson DH and Cunha BA. Drug fever. Infect Dis Clin North Am. 1996; 10(1):85-91.
Oizumi K, Onuma K, Watanabe A, et al. Clinical Study of Drug Fever Induced by Parenteral Administration of Antibiotics. Tohoku J Exp Med. 1989; 159(1): 45-56.
Hocker SE, Tian L, Li G, et al. Indicators of Central Fever in the Neurologic Intensive Care Unit. JAMA Neurology. 2013; 70(12):1499-1504.
Porat R and Dinarello CA. Pathophysiology and treatment of fever in adults. In Baron EL, ed. UpToDate. Waltham, Mass.: UpToDate, 2018. [https://www.uptodate.com/contents/pathophysiology-and-treatment-of-fever-in-adults]. Accessed Dec 26, 2018.
Often, the focus of medical education is on clinical diagnosis and management of disease. But what about prevention? Prevention is key. Here are some ways for both the patient and healthcare provider to prevent further infections:
Reduce transmission as much as possible
Wash hands with soap and water after leaving the room of a patient with active C. difficile infection (CDI) OR use an alcohol-based hand sanitizer if a sink is not available
Advocate healthcare facilities to:
place sinks nearby patient rooms
consider sink placement in the future construction of healthcare facilities
Educate your patients and those who live with them to:
wash their hands well after using the toilet
have infected individuals use separate toilets and toilet accessories during treatment, if possible
Avoid unnecessary antibiotic use
Avoid prescribing an antibiotic if low likelihood of bacterial infection
Narrow broad-spectrum antibiotics as soon as possible
Discontinue antibiotics as soon as possible
Consider prophylactic PO vancomycin for patients with history of recurrent C. difficile infection
A retrospective review demonstrated that administration of PO vancomycin 125mg twice a day was associated with a lower incidence of recurrent C. difficile infection (4.2% vs. 26.6%, p<0.001)3
Educate yourself on the risks and benefits of probiotic use and be able to relay that information to your patients if they ask.
Some studies show no reduction in incidence of C. difficile infection with probiotic use6,7
Other studies (including a Cochrane review) show significant reduction in C. difficile infection incidence with probiotic use8,9,10,11
Studies have demonstrated that probiotics are more likely to reduce C. difficile infection incidence:
in patients with a baseline risk of C. difficile infection > 5%8,9
when probiotics are administered at higher doses10
when the probiotic consists of multiple strains10
when probiotics were administered within 2 days of antibiotic initiation11
This is the IDSA Clinical Practice Guidelines for C. difficile infection statement on probiotics: “There are insufficient data at this time to recommend administration of probiotics for primary prevention of CDI outside of clinical trials (no recommendation).” The guidelines cite the bias towards probiotics in many trials that enrolled mostly patients at very high risk of C.difficile infection and the potential for probiotics to cause harm by introducing new infections to hospitalized patients.
Any prevention strategies I didn’t mention? What do you think is the most effective prevention strategy? I would love to hear your thoughts!
References
McDonald LC, Gerding DN, Johnson S, et al. Clinical Practice Guidelines for Clostridium difficile Infection in Adults and Children: 2017 Update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA). Clin Infect Dis. 2018; 66(7):1-48.
Jorgensen JH, Pfaller MA, Carroll KC, et al. Manual of Clinical Microbiology, Eleventh Edition.
Van Hise NW, Bryant AM, Hennessey EK, et al. Efficacy of Oral Vancomycin in Preventing Recurrent Clostridium difficile Infection in Patients Treated With Systemic Antimicrobial Agents. Clin Infect Dis. 2016; 63(5):651-653.
Kelly CP, Lamont JT, and Bakken JS. Clostridium difficile infection in adults: Treatment and prevention. In Baron EL, ed. UpToDate. Waltham, Mass.: UpToDate, 2018. [https://www.uptodate.com/contents/clostridium-difficile-infection-in-adults-treatment-and-prevention]. Accessed May 25, 2018.
Davidson LE and Hibberd PL. Clostridioides difficile and probiotics. In Baron EL, ed. UpToDate. Waltham, Mass.: UpToDate, 2018. [https://www.uptodate.com/contents/clostridioides-formerly-clostridium-difficile-and-probiotics]. Accessed Nov 13, 2018.
Allen SJ, Wareham K, Wang D, Bradley C, Hutchings H, Harris W, et al. Lactobacilli and bifidobacteria in the prevention of antibiotic-associated diarrhoea and Clostridium difficile diarrhoea in older inpatients (PLACIDE): a randomised, double-blind, placebo-controlled, multicentre trial. Lancet. 2013; 382(9900): 1249-57.
Ehrhardt S, Guo N, Hinz R, Schoppen S, May J, Reiser M, et al. Saccharomyces boulardii to Prevent Antibiotic-Associated Diarrhea: A Randomized, Double-Masked, Placebo-Controlled Trial. Open Forum Infect Dis. 2016; 3(1):ofw011.
Goldenberg JZ, Yap C, Lytvyn L, Lo CK, Beardsley J, Mertz D, et al. Probiotics for the prevention of Clostridium difficile-associated diarrhea in adults and children. Cochrane Database Syst Rev. 2017; 12:CD006095.
Johnston BC, Lytvyn L, Lo CK, Allen SJ, Wang D, Szajewska H, et al. Microbial Preparations (Probiotics) for the Prevention of Clostridium difficile Infection in Adults and Children: An Individual Patient Data Meta-analysis of 6,851 Participants. Infect Control Hosp Epidemiol. 2018; 39(7): 771-781.
Johnston BC, Ma SSY, Goldenberg JZ, Thorlung K, Vandvik PO, Loeb M, et al. Probiotics for the Prevention of Clostridium difficile-Associated Diarrhea. Ann of Intern Med. 2012; 157:878-888
Shen NT, Maw A, Tmanova LL, Pino A, Ancy K, Crawford CV, et al. Timely Use of Probiotics in Hospitalized Adults Prevents Clostridium difficle Infection: A Systematic Review With Meta-Regression Analysis. Gastroenterology. 2017; 152(8): 1889-1900.