This post is the second in a three-part series covering the management of beta-lactam allergies, all to be released on FOAMid over the last few months of 2019. Part 1 explained the enormous impact that penicillin allergies have on patient outcomes. Today we’ll discuss the different types of allergic reactions and the potential for beta-lactam allergy cross reactivity. Let’s jump right in!
Types of Allergic Reactions
The most common way of grouping immune-mediated hypersensitivity reactions is through the Gell & Coombs classification method.2 Using this scheme, there are four types of allergic reaction:

Type I reactions are IgE-mediated reactions and commonly referred to as immediate-type hypersensitivity reactions, since they occur minutes to hours post-exposure to an allergen. Type I reactions include anaphylaxis, angioedema, hypotension, flushing, wheezing, hives, and urticaria.
Both types II and III reactions are IgG-mediated.
Type II reactions, or cytotoxic reactions, include hemolytic anemia, thrombocytopenia, and neutropenia.
Type III reactions are immune complex reactions, and include serum sickness, glomerulonephritis, and arthritis.
Last, but certainly not least, are type IV reactions, which are T-cell mediated.
Type IV reactions are commonly referred to as delayed hypersensitivity reactions, despite Types II, III, and IV all technically being delayed in nature by days to weeks post-exposure to an allergen. A maculopapular rash, interstitial nephritis, Stevens-Johnson Syndrome (SJS), toxic epidermal necrolysis (TEN), and drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome are all considered type IV reactions.
Cross-Reactivity Risk
As discussed in the first post, many recorded antibiotic allergies are not true allergies. But when a patient does actually have a true penicillin allergy, what are the chances that the patient will have a similar reaction to other beta-lactams?
While we would generally avoid penicillins in this situation, other beta-lactams like cephalosporins and carbapenems could potentially be used. Previous studies of 10-25% cross-reactivity between cephalosporins and penicillins were primarily reported prior to 1982, when cephalosporin manufacturing processes were often contaminated with penicillin.12 Since then, the documented rate of cross-reactivity has dropped dramatically, shown in the table below.12

Cephalosporins
- Cephalosporins that do not share a side chain with penicillin have a cross-reactivity risk of <2%
- Cephalosporins that do share a similar side chain to penicillins (ex. cefoxitin and penicillin) have a cross-reactivity risk that is much higher
Side chain similarities don’t guarantee cross-reactivity, but they do increase the risk above the previously stated 2% threshold
But hold on, I thought the cause of beta-lactam allergies was the core beta-lactam ring that everyone remembers from their undergraduate years?

Not so fast. While this plays a part, more recent literature has shown that the R1 and R2 side chains also play a role in the allergy potential of cephalosporins. I have adopted and updated a table from an excellent 2008 review paper by Daryl DePestel and colleagues below.3
In this table, the 3s, 6s, and 7s stand for similar R1 or R2 side chains, as described in the cephalosporin skeleton molecule, also seen below.
- The R1 side chain is at the 7-position on the cephalosporin molecule and the 6-position on the penicillin molecule.
- The R2 side chain is at the 3-position, which only differs among cephalosporins and not penicillins.


There are a couple of important clinical points to note from this table. Probably most important for clinical practice is that cefazolin does not share side chains with any other beta-lactam agents. This can have huge consequences on the use of cefazolin in practice, especially when it comes to surgical site prophylaxis and the treatment of methicillin-susceptible Staphylococcus aureus infections, both situations that could use cefazolin as first line therapy.
And while aztreonam is known as a beta-lactam with limited cross-reactivity due to dissimilar side chains, it does actually share a side chain with ceftazidime and the more recently approved ceftolozane (marketed in combination with tazobactam).
Aztreonam & Carbapenems
Speaking of aztreonam, we’ve spent the majority of this post discussing cephalosporin cross-reactivity risk. Now let’s spend a bit of time reviewing the other agents defined in the initial table in this post: carbapenems and aztreonam. Cross-reactivity between these agents and penicillins is minimal, as seen by a number of studies published by an Italian group headed by Antonino Romano and Francesco Gaeta.4,7,9
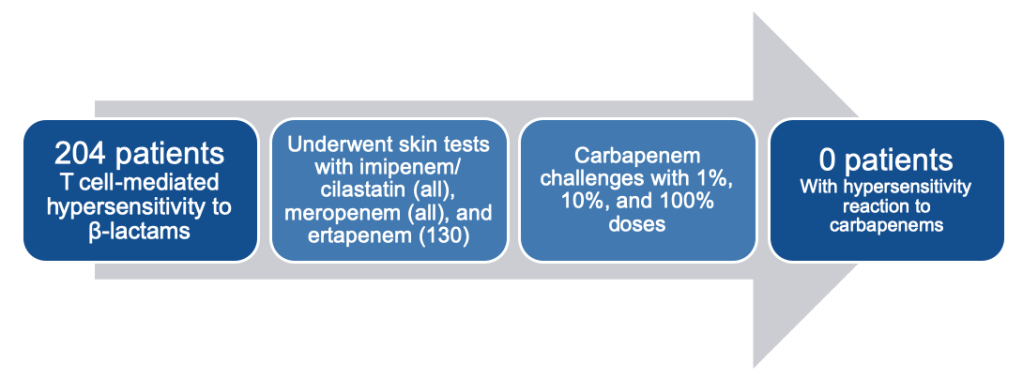
In their 2013 analysis, they found no patients had an allergic reaction to carbapenems, despite all 204 patients having a well-demonstrated T-cell-mediated hypersensitivity reaction to other beta-lactams (mostly penicillin).7
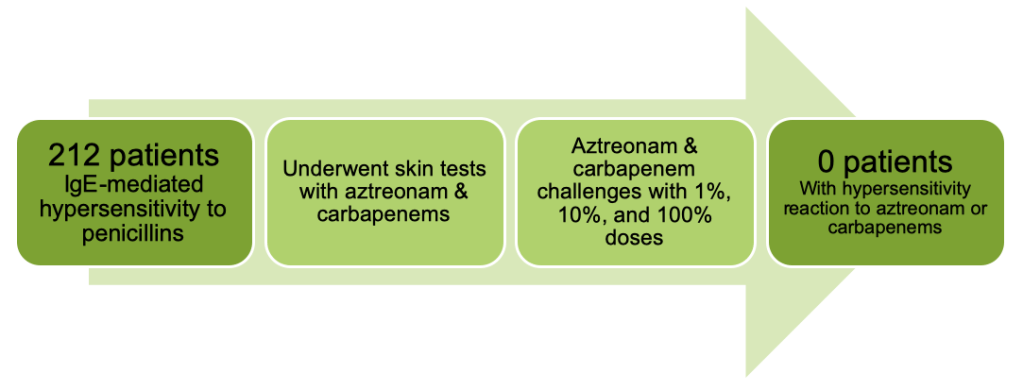
They went on to look at IgE-mediated hypersensitivity in their 2015 study, which found yet again no cases of hypersensitivity with either carbapenems OR aztreonam this time in a cohort of 212 patients with proven penicillin allergies.4
Then in 2016, they went back to T-cell-mediated hypersensitivity, examining 214 patients with proven reactions to penicillins and testing them against aztreonam. Once again, zero patients reacted to the aztreonam test doses or full dose.9

At this point, you may be questioning if the Italian group ever saw any reactions in their trial outcomes. The last study presented above that showed no reactions with aztreonam though tested more than just aztreonam. They also looked at cephalosporins and saw an 18.7% chance of positive skin testing with aminocephalosporins (cephalexin, cefadroxil, cefaclor).9 If you refer back to the previous cross-reactivity table, you can see that these three agents share a side chain with ampicillin and amoxicillin.

So while side chains play a key role in determining cross-reactivity among cephalosporins, we can be fairly confident that carbapenems and aztreonam are safe to administer in the majority of situations, especially when a non-severe penicillin allergy is documented. This will be covered in more detail in the next (and final) installment of “A Rash of Beta-Lactam Allergies,” coming to you soon!
Other posts in this series:
A Rash of Beta-Lactam Allergies, Part 1: The Problem
A Rash of Beta-Lactam Allergies, Part 3: The Solution
References
- Blumenthal KG, Peter JG, Trubiano JA, Phillips EJ. Antibiotic Allergy. Lancet. 2019; 393(10167):183-198
- Coombs P, Gell PG. Classification of allergic reactions responsible for clinical hypersensitivity and disease. In: G RR, P.G.H Gell, eds. Clinical aspects of immunology. Oxford, UK: Oxford University Press, 1968; 575-596
- Frumin J, Gallagher JC. Allergic cross-sensitivity between penicillin, carbapenem, and monobactam antibiotics: what are the chances? Ann Pharmacother. 2009; 43:304-315
- Gaeta F, Valluzzi RL, Alonzi C, Maggioletti M, Caruso C, Romano A. Tolerability of aztreonam and carbapenems in patients with IgE-mediated hypersensitivity to penicillins. J Allergy Clin Immunol. 2015; 135:972-976
- Joint Task Force on Practice Parameters; American Academy, American College, & Joint Council of Allergy, Asthma and Immunology. Drug allergy: an updated practice parameter. Ann Allergy Asthma Immunol. 2010; 105:259-273
- Legendre DP, Muzny CA, Marshall GD, Swiatlo E. Antibiotic hypersensitivity reactions and approaches to desensitization. Clin Infect Dis. 2014; 58(8):1140-1148
- Romano A, Gaeta F, Valluzzi RL, et al. Absence of cross-reactivity to carbapenems in patients with delayed hypersensitivity to penicillins. Allergy. 2013; 68:1618-1621
- Romano A, Gaeta F, Arribas Poves MF, Valluzzi RL. Cross-reactivity among beta-lactams. Curr Allergy Asthma Rep. 2016; 16:24
- Romano A, Gaeta F, Valluzzi RL, Maggioletti M, Caruso C, Quaratino D. Cross-reactivity and tolerability of aztreonam and cephalosporins in subjects with a T cell-mediated hypersensitivity to penicillins. J Allergy Clin Immunol. 2016; 138:179-186
- Romano A, Valluzzi RL, Caruso C, Maggioletti M, Quaratino D, Gaeta F. Cross-reactivity and tolerability of cephalosporins in patients with IgE-mediated hypersensitivity to penicillins. J Allergy Clin Immunol Pract. 2018; 6(5):1662-1672
- Shenoy ES, Macy E, Rowe T, Blumenthal KG. Evaluation and management of penicillin allergy: a review. JAMA. 2019; 321(2):188-199
- Trubiano JA, Stone CA, Grayson ML, et al. The 3 Cs of antibiotic allergy-classification, cross-reactivity, and collaboration. J Allergy Clin Immunol Pract. 2017; 5(6):1532-1542

2 thoughts on “A Rash of Beta-Lactam Allergies, Part 2: The Education”