This post marks part 1 of a 3-part series covering the management of beta-lactam allergies, all to be released on FOAMid over the next couple of months.
- This post, “The Problem,” provides background and the impact of a reported beta-lactam allergy
- “The Education” will delve into the types of allergic reactions, as well as cross reactivity potential among beta-lactam antibiotics
- “The Solution” will then explore how to best assess a patient’s documented allergy
With that, let’s jump right in!
Overview
A whopping 10% of the general population has a reported penicillin (PCN) allergy. But only 1-10% of these people have a true allergy when tested. This leaves us with about 0.1-1% of the general population with a true penicillin allergy.

Why is there such a discrepancy between reported allergies and true allergies? A lot of it comes from inaccurate allergy histories, like the patient with GI upset as a child, but the allergy listed as an “unknown reaction.” Or better yet, the patient whose mother had an allergy and thus everyone in the family has been given that scarlet letter in their medical record.

Another important and lesser known reason for the allergy discrepancy is that 78% of patients with immediate hypersensitivity to penicillin see their penicillin allergy fade after 10 years (from this 1981 study). So those adult patients with childhood reactions? The odds are that they aren’t still allergic decades later.
Why should we care?
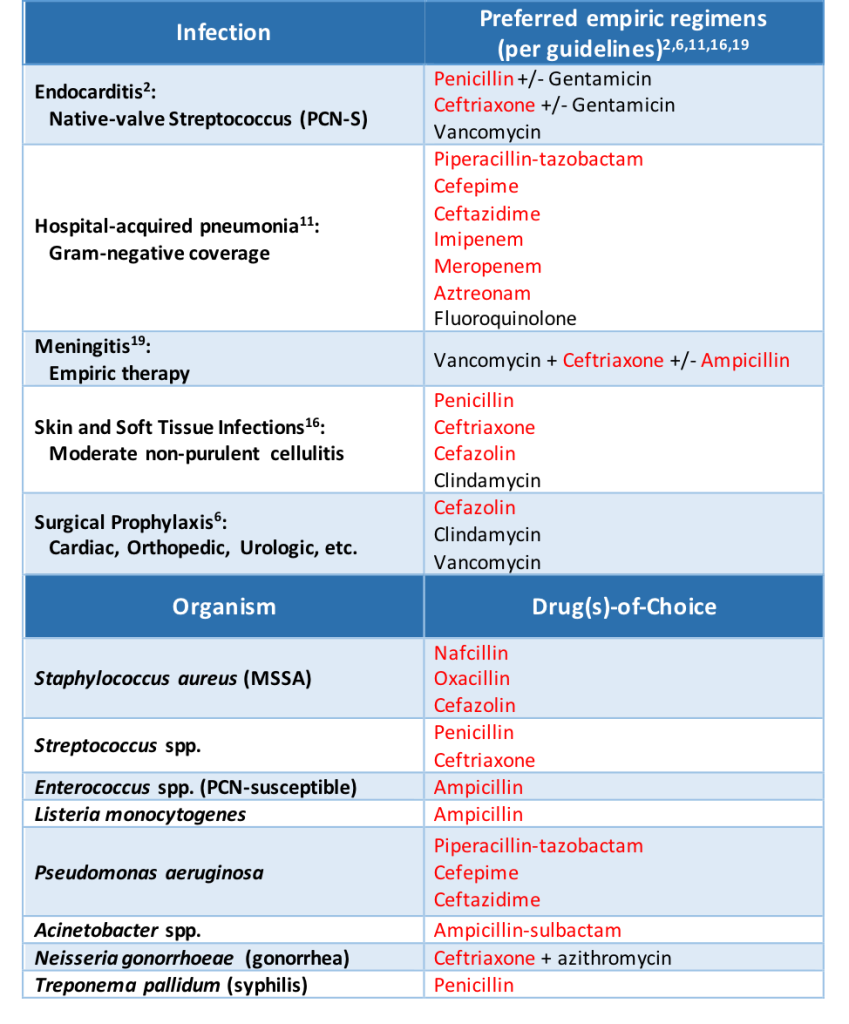
When it comes to infectious diseases, beta-lactam antibiotics are often our first- and second-line options for treatment. A documented penicillin allergy can essentially knock a practitioner down to third-line treatment in some situations. In just highlighting a few common infections and organisms, look at how often beta-lactams are brought up:
When a patient has a documented penicillin allergy, studies have proven that beta-lactam usage decreases while non-beta-lactam usage increases (Lee 2000, as well as half of the citations provided at the end of this post). And when beta-lactams are avoided, patients tend to do worse.
Impact on Patient Outcomes
The impact of a penicillin allergy is real and detrimental to our patients. Rather than bore you with paragraphs upon paragraphs detailing the many studies looking into this fact, here are some take-home points hyperlinked to the primary literature supporting the claims:
Penicillin allergy patients:
- Receive broader spectrum antibiotics, with increased use of fluoroquinolones, carbapenems, and vancomycin
- Have a longer hospital length of stay
- Have increased rates of readmission
- Have an increased risk of
- Have higher rates of clinical failure when a beta-lactam isn’t used for Gram negative bacteremia
- Have a delay in the time until they receive their first antibiotic dose
- Have higher healthcare costs
There is clear evidence that reported beta-lactam allergies pose a problem on the path to prescribing optimal treatment in infectious diseases. We can combat the issue however through education and assessment techniques.
More to come in parts 2 and 3 of “A Rash of Beta-Lactam Allergies”!
Other posts in this series:
A Rash of Beta-Lactam Allergies, Part 2: The Education
A Rash of Beta-Lactam Allergies, Part 3: The Solution
References
- Al-Hasan MN, Acker EC, Kohn JE, Bookstaver PB, Justo JA. Impact of penicillin allergy on empirical carbapenem use in gram-negative bloodstream infections: an antimicrobial stewardship opportunity. Pharmacotherapy. 2017; 38(1):42-50
- Baddour LM, Wilson WR, Bayer AS, et al. Infective endocarditis in adults: diagnosis, antimicrobial therapy, and management of complications: a scientific statement for healthcare professionals from the American Heart Association. Circulation. 2015; 132:1435-1486
- Blumenthal KG, Lu N, Zhang Y, Li Y, Walensky RP, Choi HK. Risk of meticillin resistant Staphylococcus aureus and Clostridium difficile in patients with a documented penicillin allergy: population based matched cohort study. BMJ. 2018; 361:k2400
- Blumenthal KG, Ryan EE, Li Y, Lee H, Kuhlen JL, Shenoy ES. The impact of a reported penicillin allergy on surgical site infection risk. Clin Infect Dis. 2018; 66(3):329-336
- Borch JE, Andersen KE, Bindslev-Jensen C. The prevalence of suspected and challenge-verified penicillin allergy in a university hospital population. Basic Clin Pharmacol Toxicol. 2006; 98:357-362
- Bratzler DW, Dellinger EP, Olsen KM, et al. Clinical practice guidelines for antimicrobial prophylaxis in surgery. Surg Infect. 2013;14(1):73-156
- Charneski L, Deshpande G, Smith SW. Impact of an antimicrobial allergy label in the medical record on clinical outcomes in hospitalized patients. Pharmacotherapy. 2011; 31(8):742-747
- Conway EL, Lin K, Sellick JA, et al. Impact of penicillin allergy on time to first dose of antimicrobial therapy and clinical outcomes. Clin Ther. 2017; 39(11):2276-2283
- Huang KHG, Cluzet V, Hamilton K, Fadugba O. The impact of reported beta-lactam allergy in hospitalized patients with hematologic malignancies requiring antibiotics. Clin Infect Dis. 2018; 67(1):27-33
- Jeffres MN, Narayanan PP, Shuster JE, Schramm GE. Consequences of avoiding β-lactams in patients with β-lactam allergies. J Allergy Clin Immunol. 2016; 137(4):1148-1153
- Kalil AC, Metersky ML, Klompas M, et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis. 2016; 63(5):e61-e111
- Lee CE, Zembower TR, Fotis MA, et al. The incidence of antimicrobial allergies in hospitalized patients: implications regarding prescribing patterns and emerging bacterial resistance. Arch Intern Med. 2000;160(18):2819-2822
- Macy E, Ngor EW. Safely diagnosing clinically significant penicillin allergy using only penicilloyl-poly-lysine, penicillin, and oral amoxicillin. J Allergy Clin Immunol Pract. 2013; 1:258-263
- Macy E, Contreras R. Health care use and serious infection prevalence associated with penicillin “allergy” in hospitalized patients: A cohort study. J Allergy Clin Immunol. 2014; 133(3):790-796
- Solensky R. The time for penicillin skin testing is here. J Allergy Clin Immunol Pract. 2013; 1(3):264-265
- Stevens DL, Bisno AL, Chambers HF et al. Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America. Clin Infect Dis. 2014; 59(2):e10-e52
- Sullivan TJ, Wedner HJ, Shatz GS, Yecies LD, Parker CW. Skin testing to detect penicillin allergy. J Allergy Clin Immunol. 1981; 66(3):171-180
- Trubiano JA, Chen C, Cheng AC, et al. Antimicrobial allergy ‘labels’ drive inappropriate antimicrobial prescribing: lessons for stewardship. J Antimicrob Chemother. 2016; 71:1715-1722
- Tunkel AR, Hartman BJ, Kaplan SL, et al. Practice guidelines for the management of bacterial meningitis. Clin Infect Dis. 2004; 39:1267-1284
- van Dijk SM, Gardarsdottir H, Wassenberg MW, Oosterheert JJ, de Groot MC, Rockmann H. The high impact of penicillin allergy registration in hospitalized patients. J Allergy Clin Immunol Pract. 2016; 4:926-931

2 thoughts on “A Rash of Beta-Lactam Allergies, Part 1: The Problem”